[OPINION]: Generative AI and I, by Abdalla Uba Adamu
By Abdalla Uba Adamu
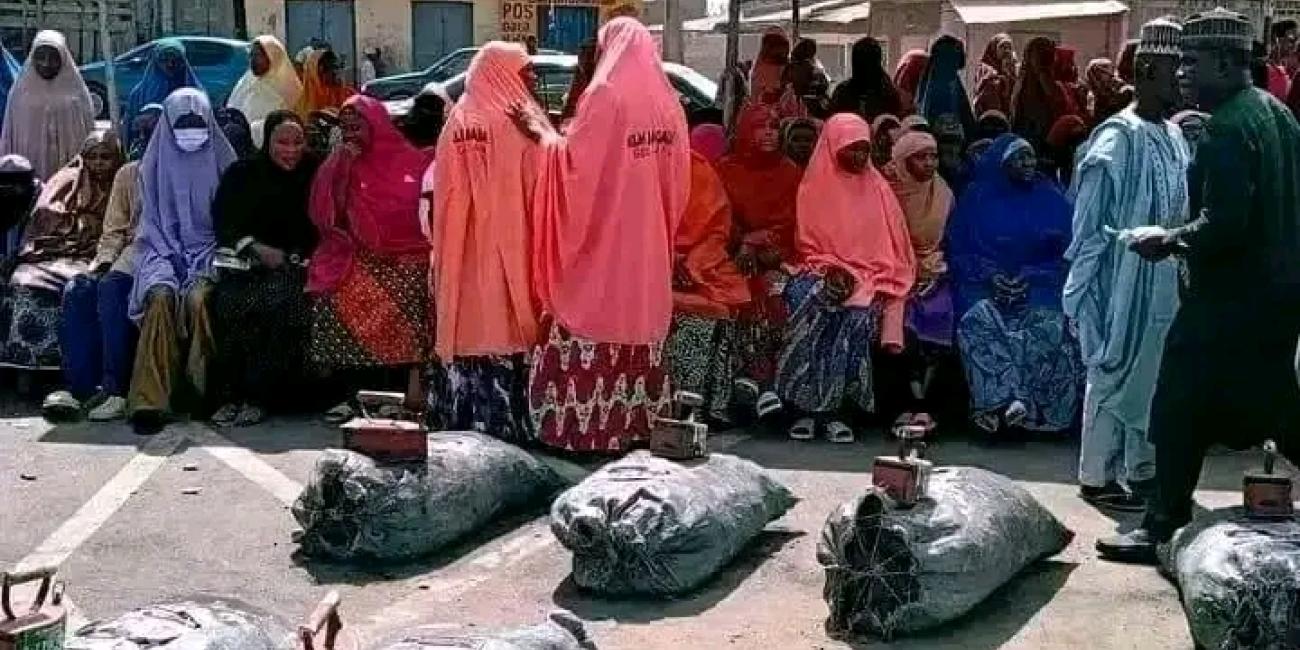
My most recent post on the Hausa traditional technologies of cloth-making and weaving raised a very interesting—and very welcome—comment: did I use AI to write the post? The simple answer is no. Now, let me unpack the issue (and while this sentence is not AI-generated, it is definitely AI-syntax!!!).
I have noticed over several weeks postings that are definitely AI by people whose writing I am quite familiar with. You get to notice these things after almost half-century of teaching and supervising student projects and dissertations at all level, and all in the English language. Words that keep popping up in these recent postings include: “ecosystem”, “DNA”, “spine”, “architecture”, “chamber”, “leverage”, “cartography”, “nuance”, “cascade”, and of course, “unpack.”
Generative AI produces prose in a neat, grammatically correct and often archaic language. When someone is not used to writing in that syntax and they suddenly do, then it is AI at work. And words that don’t belong in normal conversation. For God’s sake, how frequently do you use “ecosystem” or “DNA”? But suddenly they begin to appear in someone’s writing! Even if it is not directly AI, you were subtly influenced by AI Grammar!
Further, AI can produce perfect grammar and spelling, but the content often lacks depth or original insight. Do you see spelling errors or factual mistakes? That’s human, not AI. Do you see polished perfect grammatically error-free narrative? Suspect, but not always, AI, especially if the person is not a seasoned or regular writer.
As I assured my commenter, none of my postings has ever been written by AI, nor will it be. Every word, comma and period are made by me in Ɗorayi Babba, Kano! My writing might seem like AI simply because I use an academic register in my normal writing. In other words, ingantaccen turanci, which the AI machine is not used to seeing in social media posts. AI detectors are guessing probabilities—not identifying authorship. I write very carefully, going over what I write at least three times, checking facts, spelling, context, before I press the send paper airplane icon (I also use my laptop for all postings, to avoid mistakes as much as possible).
Pick any of my writings from, say 2001, dump it in AI, it will tell you it was AI-written. This was before the Generative version of AI became commodified social conversations. Thus, in an academic writing AI will not flag my writing. But it might in social media posting because the AI checker will expect a loose, public-oriented syntax. Look for “human flags” in all my writings. In the post in question, the flag is: “Remove the cloth—and we revert back to our animal origins. Our shame exposed, because we are now aware.” No AI will write that because it is a human thought, expressed by a human. In fact, it even tells you that the human is religious—invoking religious imagery to make a point. AI is religiously, spiritually and politically neutral—except Grok!
The passage refers to the awareness Prophet Adam (AS) of his nakedness after eating the Forbidden Fruit in Paradise. The leaf he used to cover himself is now the clothe the picture glorifies—the civilizational tool which separates us from animals that are naked. That is religious philosophy. No AI can come up with this insight.
So, do I use AI? Referring of course to Generative AI. Of course! In 2026 any person NOT using AI is in serious trouble in the global knowledge economy, in any sphere. I use the paid version which gives me more features (I will not tell you which AI I use so as not to advertise free for them!).
If I am asked to write a chapter for a book or a journal article, I never use AI for the main prose. I use it only to gather titles of reference materials (and I then fly to the Acibilistan Central Library, using Acibilisian Airways, to borrow copies), and I doubly verify the references are real, not AI-hallucination (I have caught it on one or two occasion, and I “warn” it never to give me what it thinks I want; only what is real). But the prose is mine. Funnily enough, even the AI I used is quietly impressed with the titles of my projects—go over my past publications and you will what I mean—and this was before the Generative AI revolution.
I don’t even use it for my lectures. I may ask for lecture outline—and promptly decline any offer of writing the lecture notes. The reason is that all my lectures are based on my ethnographic field experiences—with actual examples of videos, photos, or experiences shared with my students at all levels.
Other cases where I allow AI to draft something for me might be where I am asked on a short notice to be a keynote speaker. But give me weeks’ notice in advance, I cook my own meal. Or write reference for someone. When it produces the draft, I go over it and input personal touches. (it will write, “he is a hard worker”, I will write, “he is an excellent co-worker and sociable person whom I have known for over ten years”).
One ongoing case where I use the AI is in editing my autobiography, and I find it tremendously useful at that. I have written more than 90% of the book, given it to human editors to correct, mainly article misplacement, grammar etc. Once I subscribed to the paid version of my AI, I send it the previous chapters (which, unwisely, were written in Third Person, but that’s a story for another day). It converted everything to the First Person POV I asked it to. Then it smoothened sentences, polished passages, but, and I warned it right from the beginning, did not add anything. I always use it in editorial mode. Save me lots of money from human editors (and time chasing them for return)! It has an often irritating tendency to lead you to a rabbit hole, but I always claw my way out of it. So, my Prompts tell it to be Editorial, not Authorial. It is a nice relationship that keeps the integrity of my words, and saves me a lot of money in paying human editors to edit the work.
I am happy that people are beginning to notice the increasing rise—and use— of Generative AI, even trying to pinpoint it. This is good. Equally happy that some AI tools are capable of answering Prompts in the Hausa language—thus opening up the Hausaphone world to the global knowledge economy.
Now, I ask you. Do you use Generative AI? In what ways. Are you happy with it, or do you feel you are surrendering your intellect to a machine? Or are you Die Mensch-Maschine (ask your AI to translate that!)?
Abdalla Uba Adamu
Department of Information and Media Studies
Faculty of Communication
Bayero University Kano
March 10, 2026